Challenges and Opportunities in Inflammatory Breast Cancer
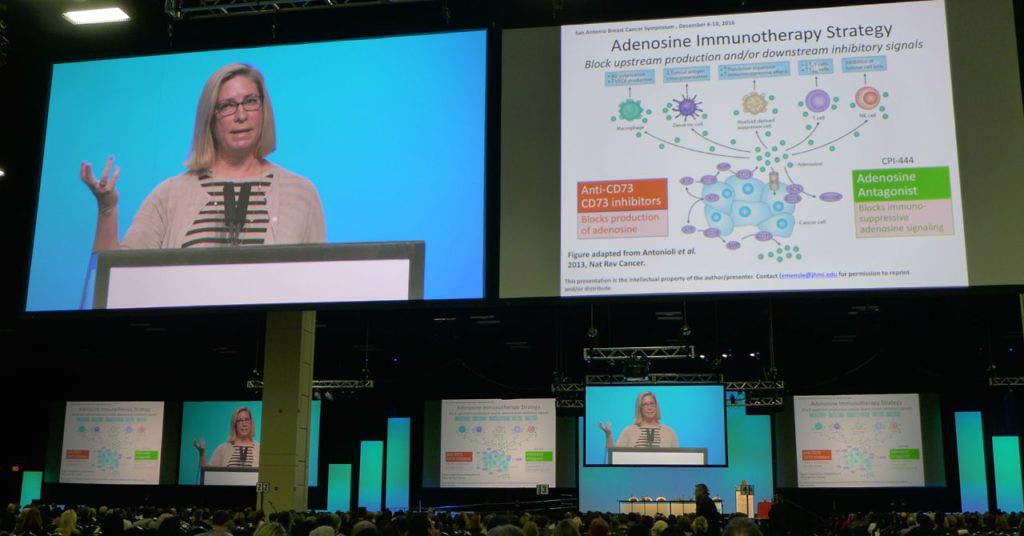
At the 2016 San Antonio Breast Cancer Symposium (SABCS16), I had the great pleasure to talk with a leading inflammatory breast cancer expert and translational researcher, Naoto T. Ueno MD PhD.

Dr Naoto Ueno at SABCS16
Dr Ueno is Executive Director of the Morgan Welch Inflammatory Breast Cancer Research Program and Clinic at the University of Texas MD Anderson Cancer Center.
He’s active on Twitter where, as @teamoncology, he shares information on the latest developments in breast cancer, often writing in Japanese for his followers.
A cancer survivor himself, he also brings an empathy to patient care through his own treatment experience.
Anyone who follows him on Twitter, will also know he is a “foodie.” Prior to our chat, I joked he should write the definitive guide to San Antonio restaurants for attendees… he definitely ate better than I did at the meeting!
MD Anderson also has an IBC conference coming up next month for those interested in the area:
Join the Inflammatory Breast Cancer Conference on 2/11 & 12. Learn the latest info to cure IBC. Brochure→ https://t.co/EyejRO0fRR #endcancer
— Naoto Ueno, MD, PhD (@teamoncology) December 21, 2016
What caught my attention at SABCS16 were posters from MD Anderson researchers that offered insight into the challenges and opportunities in targeting this rare form of breast cancer, something we don’t hear a lot about.
Subscribers can login to read the interview Dr Ueno kindly gave BSB. This is the fourth in our series of expert interviews from San Antonio.
If you have a keen interest in IBC, do follow @teamoncology – if you don’t already!
This content is restricted to subscribers

 It also heralded a great lineup of cancer researchers largely characterised by unconventional thinking. This, of course, is a good thing because it is only by dismissing dogma that a field can move forward unconstrained.
It also heralded a great lineup of cancer researchers largely characterised by unconventional thinking. This, of course, is a good thing because it is only by dismissing dogma that a field can move forward unconstrained.
 A bunch of my Post Doc chums in this field were at the San Antonio Breast Cancer Symposium (SABCS) meeting and gleefully highlighted mobbed posters or areas where they thought the data looked potentially interesting.
A bunch of my Post Doc chums in this field were at the San Antonio Breast Cancer Symposium (SABCS) meeting and gleefully highlighted mobbed posters or areas where they thought the data looked potentially interesting. At SABCS a couple of things looked pretty intriguing indeed. One we will cover in the New Year, along with an in-depth expert interview on the topic, while the other is the main focus of today’s note.
At SABCS a couple of things looked pretty intriguing indeed. One we will cover in the New Year, along with an in-depth expert interview on the topic, while the other is the main focus of today’s note.