Head and Neck cancer – or to be more precise – squamous cell carcinoma of the head and neck (SCCHN) has joined the checkpoint inhibitor club with two FDA approvals this year. 
Firstly, we saw the accelerated approval of pembrolizumab (Merck) based on objective response rate on August 5, 2016 for patients with recurrent or metastatic head and neck squamous cell carcinoma (SCCHN) that has continued to progress despite standard-of-care treatment with chemotherapy.
It’s a dismal disease with a generally poor prognosis in advanced patients once initial therapy fails.
While some patients do benefit with anti-PD–1 checkpoint therapy, the overall response rate in the KEYNOTE–012 trial of 174 patients was pretty low, i.e. 16%. In other words, the majority of patients do not respond or receive any clinical benefit.
Secondly, last week on November 10 nivolumab (BMS) was approved by the FDA based on the phase 3 CheckMate–141 data presented at ASCO earlier this year. The data was published in the New England Journal of Medicine to coincide with the FDA approval.
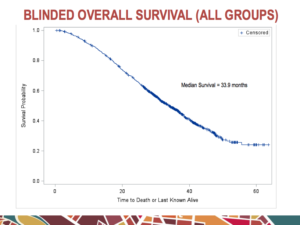
There were no statistically significant differences between the two arms for median PFS (2.0 months with nivolumab versus 2.3 months with standard therapy, HR for disease progression or death, 0.89; P=0.32) or ORR (13.3% vs. 5.8%) for nivolumab versus investigator’s choice, respectively. There was, however, a clear benefit in favour of nivolumab in median overall survival (7.5 months in the nivolumab group versus 5.1 months in the control group; HR 0.70; P=0.01).
This effect on patient outcome is a classic pattern for cancer immunotherapy with checkpoint blockade. Response rate and PFS are measurements that are very relevant to chemotherapy, but they are not as relevant to cancer immunotherapies where what is impacted more noticeably is overall survival and the long tail of the curve.
With two approved anti-PD–1 monotherapies in SCCHN, the next challenge has now become how can we improve on monotherapy by boosting the number of PRs to CRs potentially improving long term outcomes and/or turn non-responders into responders? This is the stage we are at in many tumour types now.
Combination approaches are believed to be the way forward, which is why we anticipated with great interest the lirilumab plus nivolumab head & neck combination data presented this past weekend at the 2016 Society for Immunotherapy of Cancer (SITC) meeting at National Harbor, MD. The presentation is available for download on the Innate Pharma website. The data raises numerous questions and scenarios that can be considered…
- Are the data exciting, encouraging or disappointing?
- Are the results enough to give confidence if a phase 3 trial with the combination were to follow?
To address these questions and other critical issues – including red and green flags – we took a deep dive into the data in the context of scientific facts and explored the landscape carefully.
To learn more insights, Subscribers can log in for more details…
This content is restricted to subscribers


 Before we get into our in-depth coverage based on the tumour type, target and modality landscapes, I wanted to take a moment to highlight five key abstracts that stood out for me as worthy of checking out in more detail once we get to Chicago.
Before we get into our in-depth coverage based on the tumour type, target and modality landscapes, I wanted to take a moment to highlight five key abstracts that stood out for me as worthy of checking out in more detail once we get to Chicago. Indeed, at the ASCO-SITC meeting in Orlando last week, another such target emerged and clinical evaluation is already underway, making it a worthwhile area to explore.
Indeed, at the ASCO-SITC meeting in Orlando last week, another such target emerged and clinical evaluation is already underway, making it a worthwhile area to explore.
