Yesterday saw the FDA approval of atezolizumab (Tecentriq) for the second-line treatment of metastatic non-small cell lung cancer (NSCLC) (link to company press release). According to Genentech:
“This approval is based on results from the randomized Phase III OAK and Phase II POPLAR studies. The largest study, OAK, showed that TECENTRIQ helped people in the overall study population live a median of 13.8 months, 4.2 months longer than those treated with docetaxel chemotherapy (median overall survival [OS]: 13.8 vs. 9.6 months; HR = 0.74, 95% CI: 0.63, 0.87). The study enrolled people regardless of their PD-L1 status and included both squamous and non-squamous disease types.”
The FDA approval is largely a broad one in 2L and 3L across PD-L1 expression and histologies [Link]:
“TECENTRIQ is indicated for the treatment of patients with metastatic non-small cell lung cancer (NSCLC) who have disease progression during or following platinum-containing chemotherapy. Patients with EGFR or ALK genomic tumor aberrations should have disease progression on FDA-approved therapy for these aberrations prior to receiving TECENTRIQ.”
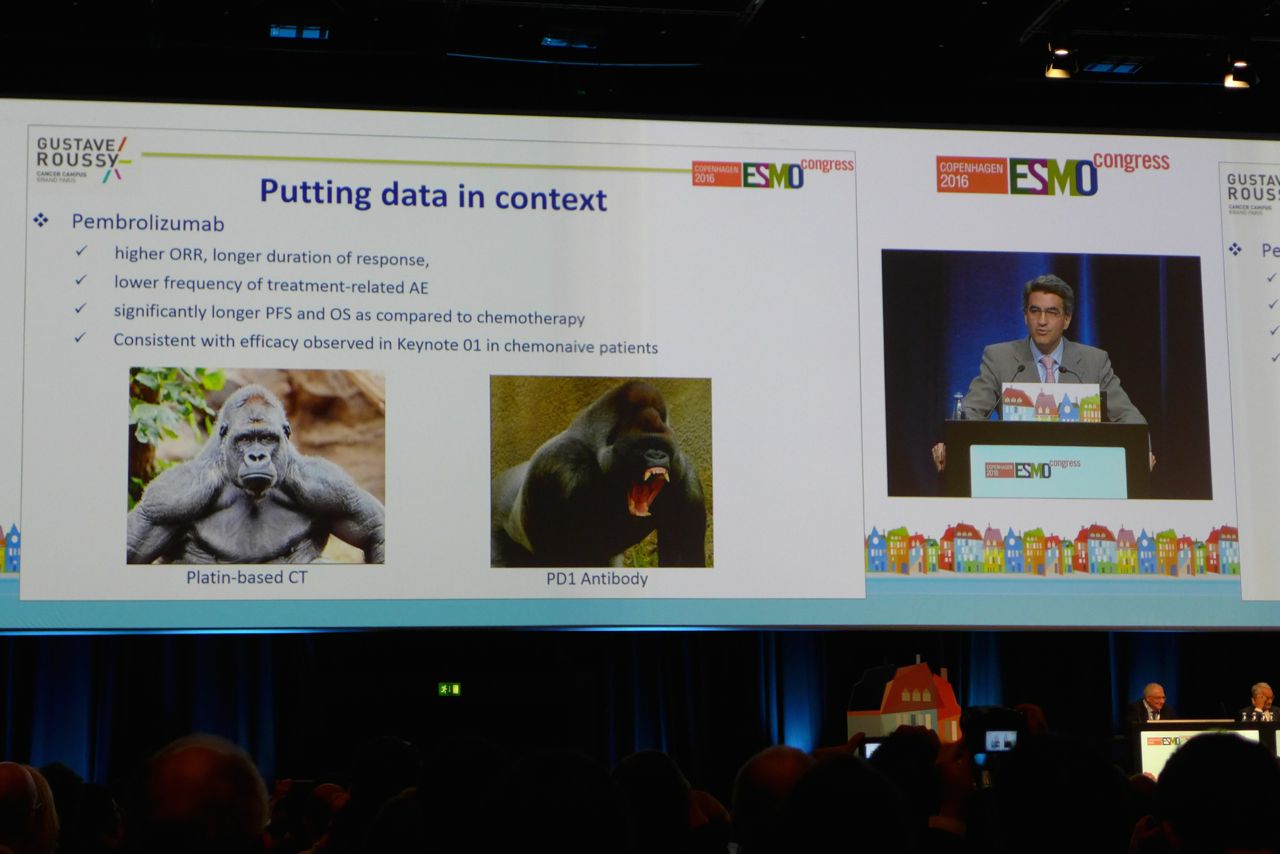
The approval was widely expected in light of the Phase III OAK trial data presented in the Presidential Symposium at ESMO16 meeting in Copenhagen.

Sign adjacent to #ESMO16 in Copenhagen
Imagine hearing live about positive first-line data with pembrolizumab, with and without chemotherapy, negative data from nivolumab in the same setting, the 2L data for atezolizumab and two discussants drilling into both the data and broader impact of these studies to a jam packed audience that even included thought leaders from other tumour types who were also eager to hear the news. To say the atmosphere was electric would be a rather British understatement here.
We previously covered our initial impressions from that session [Link], but we also had the pleasure and privilege of interviewing a leading US thought leader in the lung cancer space after the session to garner his impressions of the data and also some perspectives on the key issues that the field is facing.
The pembro plus chemo data is already providing some controversy amongst various protagonists given there are a number of similar combination trials expected to read out over the next year to 18 months, plus much anticipation from analysts regarding the ditching of chemo for IO combos such as anti-PD–1 plus anti-CTLA–4 (BMS and AstraZeneca have keen stakes here), but what do thought leaders really think of that concept? Is that the slam dunk that many analysts seem to think it is?
This, my friends, is where things start to get a lot more complicated, akin to 3D chess in Star Trek.
What is happening now in advanced NSCLC is not how the market will look in a year or two. In many ways, the rate of approvals are outstripping the pace of science right now, but once the low hanging fruit is gone, competition will need to evolve in much more sophisticated and elegant levels.
With these questions in mind, we have a double header for you today – you can read on to find out more details from our latest though leader interview, supported by some insightful perspectives from a medical oncologist who treats lung cancer patients in private practice. Today’s post therefore covers some wide ranging discussions across the key issues in advanced NSCLC and it’s future direction.
Subscribers can log-in to learn more insights
Please note that subscription prices will increase on Monday 24th, so if you’ve been on the fence about our upcoming coverage of #SITC2016, #ENA2016 (EORTC/NCI/AACR Mol Targets), #ASH16, #SABCS16 and #JPM17 then now is a good time to lock in at the current rates!
This content is restricted to subscribers

 Our extensive reviews and discussions in this area have included a look at:
Our extensive reviews and discussions in this area have included a look at: