What Tesaro aren’t telling you about niraparib
Copenhagen – PARP inhibitors are creating quite a lot of controversy here at the 2016 ESMO Congress.
Yesterday, we heard the data for rucaparib (Clovis Oncology) as monotherapy treatment for the advanced ovarian cancer patients with BRCA mutations who have been treated with 2 or more chemotherapies.
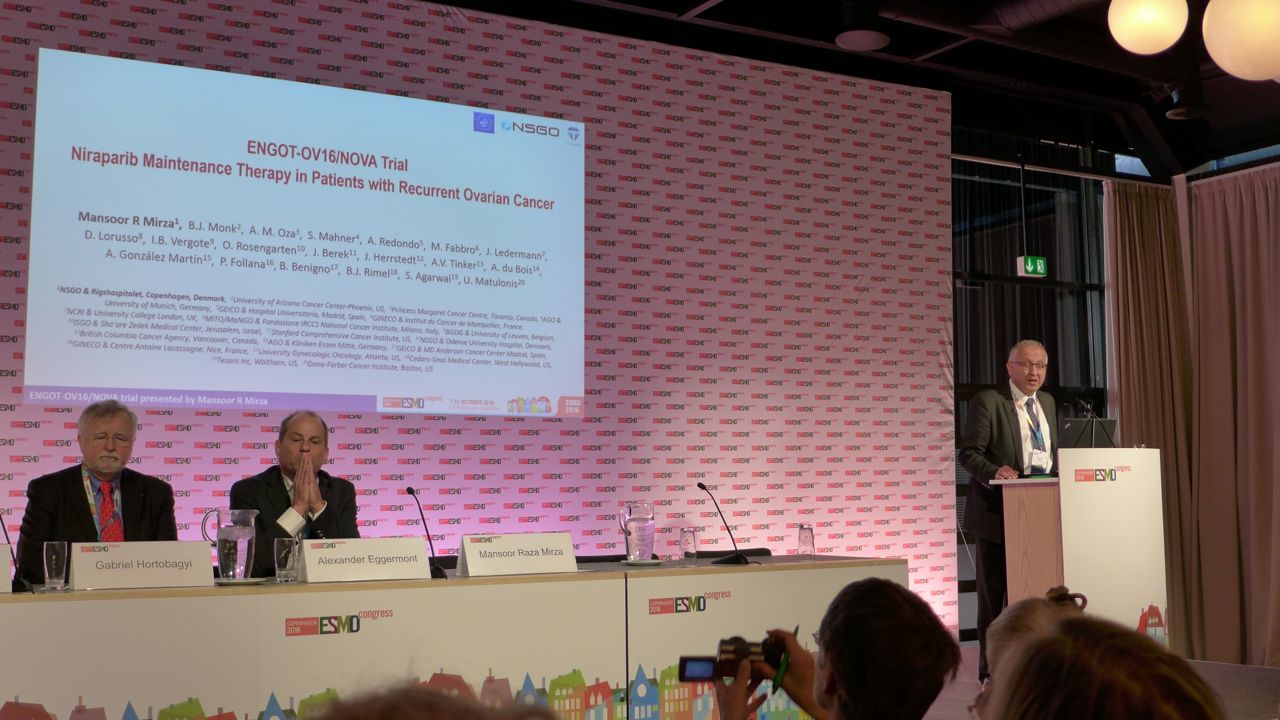
In a totally different ovarian cancer indication, today at #ESMO16 we heard the results of the phase 3 trial for niraparib, the PARP inhibitor from Tesaro, that many thought was superior to the rucaparib data, ignoring the fact you can’t make comparisons for maintenance versus relapsed/refractory treatment.
The niraparib ENGOT trial was presented in today’s plenary Presidential Symposium by Dr Mansoor Mirza and simultaneously published in The New England Journal of Medicine (link). It was also featured in a media briefing earlier today in Copenhagen.
In this piece we’ve taken a critical look at the Tesaro (NASDAQ: TSRO) niraparib data and the controversial claim made by their principal investigator, Dr Mirza, that the data shows there is no need for a companion diagnostic to be associated with this drug.
In other words, the intent that regulatory approval will be sought for this drug as maintenance therapy for platinum-sensitive ovarian cancer patients, irrespective of whether they have a BRCA mutation or homologous recombination deficiency (HRD).
This post provides commentary on this and offers the perspective of a leading ovarian cancer expert with deep experience of companion diagnostics in this field.
Subscribers can login to read what Tesaro aren’t saying about the Niraparib data or you can purchase access…
This content is restricted to subscribers
 Today’s news that an FDA Oncologic Drugs Advisory Committee (ODAC) review will not be required for rucaparib is good news for Clovis Oncology. The company announced this via an SEC 8K filing:
Today’s news that an FDA Oncologic Drugs Advisory Committee (ODAC) review will not be required for rucaparib is good news for Clovis Oncology. The company announced this via an SEC 8K filing: When it comes to cancer immunotherapy drug development, one of the challenges is that we can’t accurately predict from preclinical mouse models what will happen in people. The result is a rush into the clinic to test in human subjects.
When it comes to cancer immunotherapy drug development, one of the challenges is that we can’t accurately predict from preclinical mouse models what will happen in people. The result is a rush into the clinic to test in human subjects.